the problem
retinopathy of prematurity (ROP) is a condition where abnormal blood vessels grow in the retinas of babies born before 36 weeks or under 1,500g. left untreated, those vessels contract and pull the retina off the back of the eye. permanent blindness.
here's the thing: if you catch it early, laser therapy can prevent vision loss entirely. the problem is that the screening cameras that do this cost $14k–$125k, require a trained ophthalmologist to operate, and are too bulky to move between hospitals. in countries like kenya. where neonatal survival rates have jumped, but specialist infrastructure hasn't kept up. countless infants go undiagnosed.
design an affordable, portable retinal screening device that a neonatal nurse with one hour of training can use. so hospitals in low-resource settings can finally screen for ROP before it's too late.
by the numbers
the camera is already sufficient for detecting plus disease. the vessel dilation and tortuosity in zone I that signals ROP. zone I is where the disease is most dangerous, and our static image captures it cleanly. future iterations will use image stitching to push the FOV past 120° (the full ISO target for ROP screening).
the device
the final prototype is a handheld 3D-printed tube that integrates four parts: a high-output warm LED for illumination, a 28D ophthalmic lens for magnification, a 64MP arducam owlsight camera, and a raspberry pi zero 2W for capture and control.
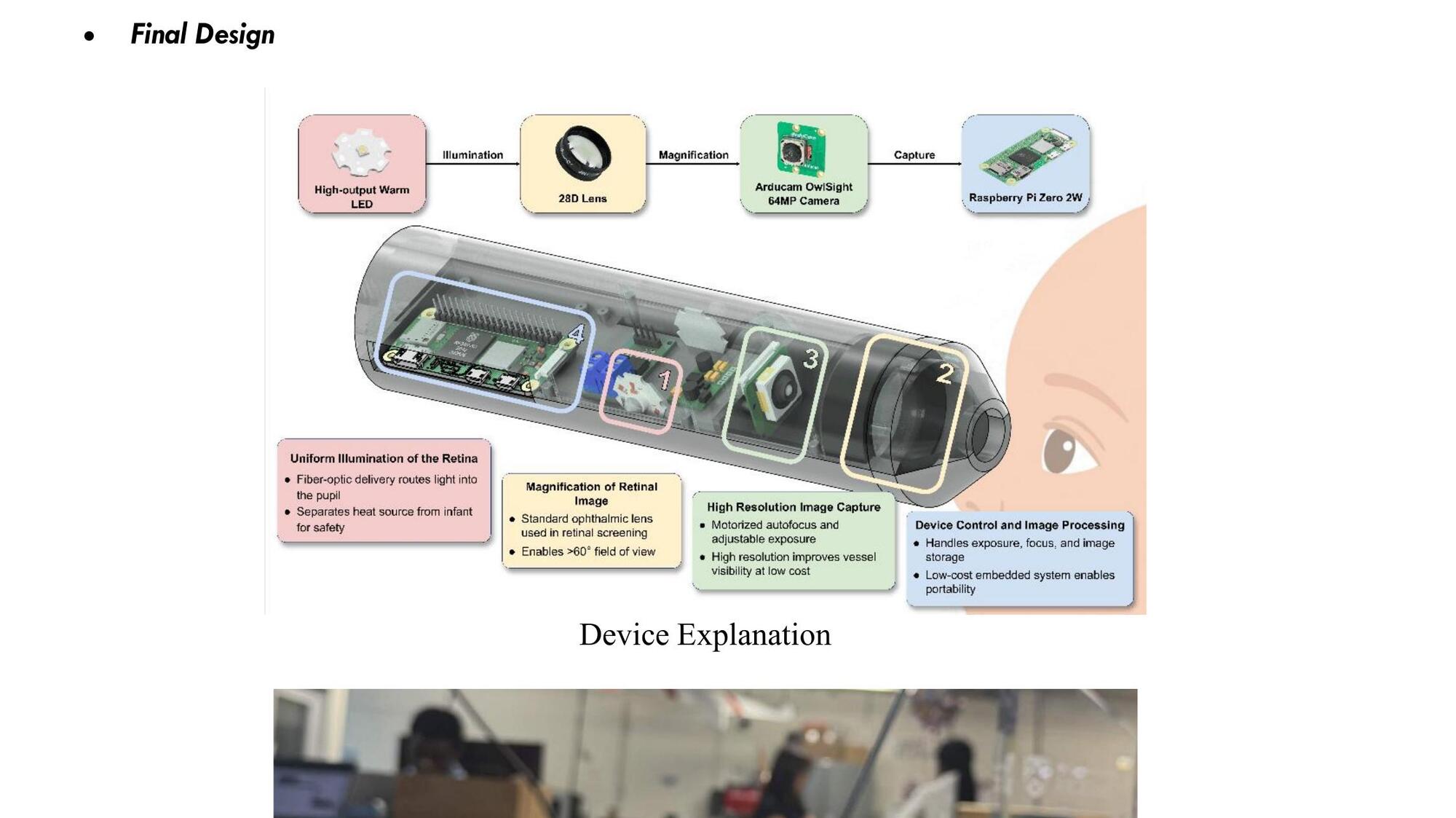
the four components, from pupil to processor
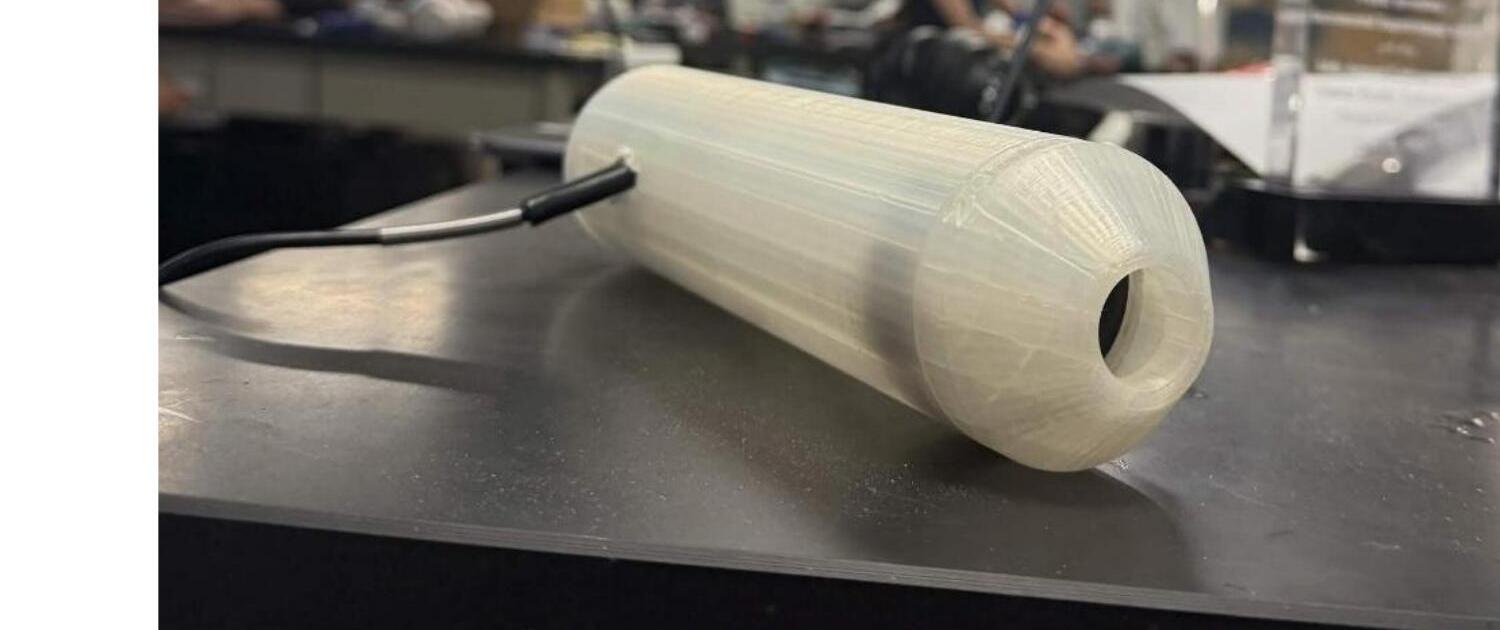
the assembled device: single-piece 3d printed housing, swappable front cone
the app
a companion app pairs with the device so a nurse can capture, label and review screenings without ever leaving the patient. it supports english and kiswahili, manages patient records, and gives a live preview during capture.
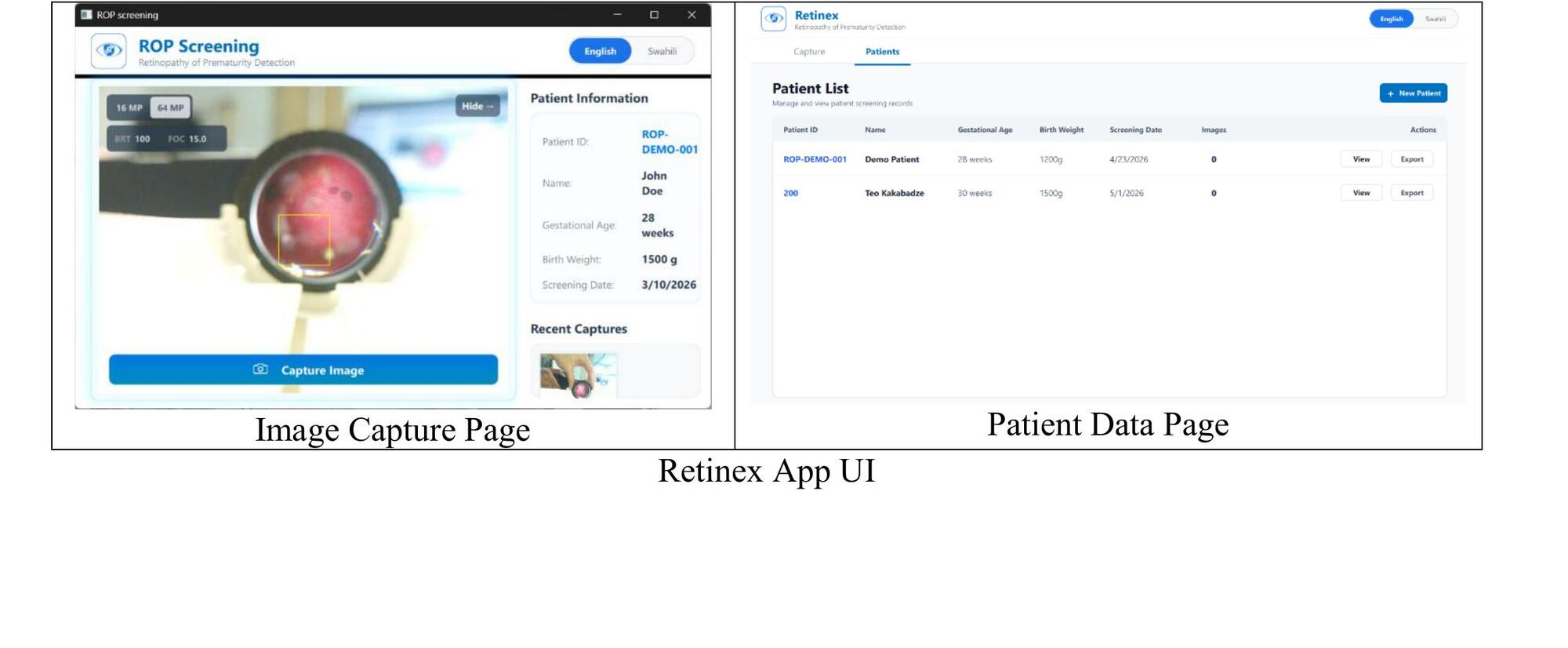
image capture (left) and patient management (right)
the journey
we inherited a prototype called IRIS from a previous EDES 120 team. it was a great starting point but had a few critical issues: bulky casing, external lighting causing glare, blunt front end that made pupil alignment hard, low camera resolution. so we redesigned around those.
inherited prototype analysis
tested the IRIS prototype and ran its AI model. measured baseline resolution at 8.0 lp/mm. far below clinical needs. identified key failure points.
medium-fidelity prototype
my main contribution: designed and CADed a smaller, ergonomic housing with autofocus and a higher-resolution camera. measured 32 lp/mm, a 4× jump from IRIS.
final prototype
refined optics, added warm LED + off-axis lighting prototype, tuned autofocus, integrated the raspberry pi. final resolution: 35.9 lp/mm, FOV 60–80°, plus disease detection working.
handoff to client
delivered working device + documentation to our client katherine sammy, and handed off all materials for the next team.

where we started: the inherited IRIS prototype
mid-cycle redesign: smaller, ergonomic, autofocus
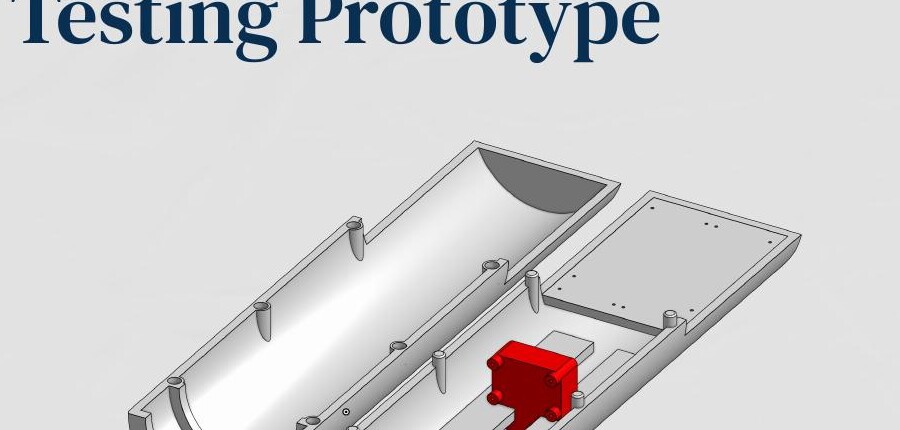
testing
i designed and CADed a custom testing rig that holds the prototype, slides the camera for focus testing, and aligns it precisely with a USAF 1951 resolution target the standard for measuring optical resolution.
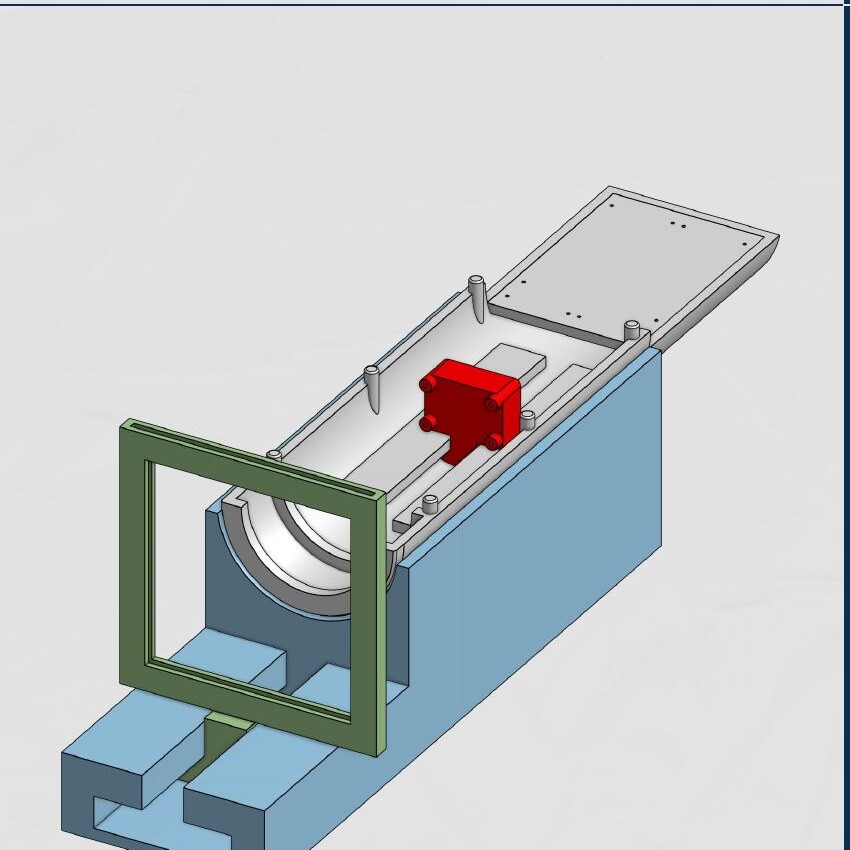
testing rig: gray = prototype holder, red = camera slider, blue = base, green = test plate holder
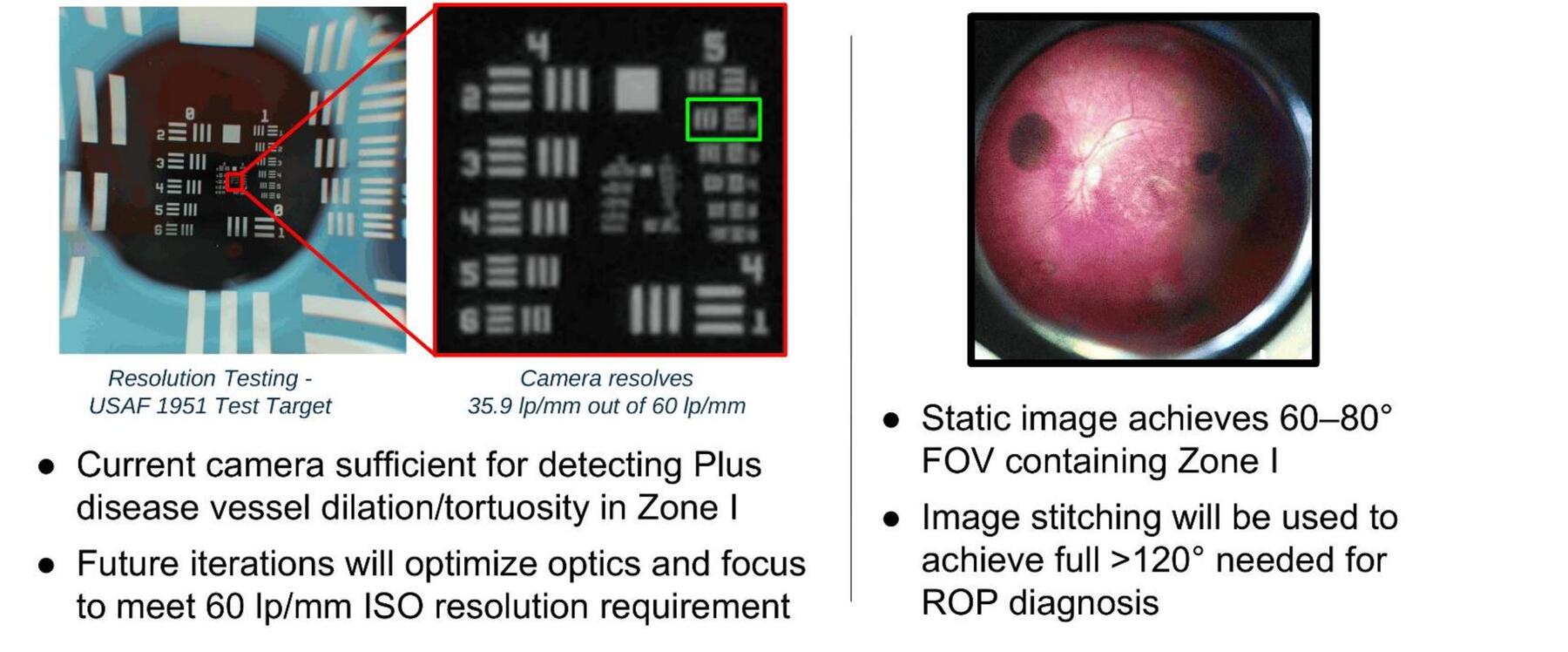
final resolution test (35.9 lp/mm) and a captured retina image with 60–80° FOV containing zone I
what i worked on
i focused on the hands-on engineering side: the physical device and the test infrastructure.
- cad + mechanical design. designed every iteration of the housing, internal mounts, ergonomic form factor, and the swappable front cones.
- prototyping. built and assembled the physical prototypes: fit, tolerance, integration of the camera, lens and pi inside the casing.
- testing rig design. the entire rig: prototype holder, adjustable camera slider, base and integrated x-axis test plate holder.
- optical testing. ran the USAF 1951 resolution tests, documented results, iterated on the optics.
- optics research. contributed to lens selection and modeling the premature infant eye geometry.
bill of materials
under $500 was our target. we landed at $154.64.
| component | cost |
|---|---|
| arducam owlsight 64MP camera | $55.99 |
| pocketretina 28D BIO lens | $49.99 |
| raspberry pi zero 2W | $15.00 |
| 3W high-output LED | $10.19 |
| buck-boost converter | $9.99 |
| fiber optic cables | $7.99 |
| high-power MOSFET trigger switch | $5.49 |
| total | $154.64 |
what's still hard
we shipped a working prototype but we're not pretending it's done. these are the real challenges the next team will pick up:
- no real-world clinical validation yet. we tested on a model retina. dilated infant eyes will behave differently: movement, pupil response, the works. clinical validation through IRB approval is the most important next step.
- off-axis lighting is a workaround. coaxial lighting (like commercial devices use) needs a beamsplitter that costs thousands of dollars in quality components. our off-axis prototype works but needs tuning of the ring angle and ideally a larger-diameter fiber optic cable.
- focus distance bottleneck. the camera has a 12 cm minimum focus distance, which means ~15 cm of wasted space inside the tube. swapping in a different sensor with a shorter minimum could reclaim that.
- autofocus tuning. the autofocus settle time and fine clarity still need adjustment for the screening workflow.
- FOV to 120°. the static image hits 60–80°. getting to the full 120° needed for ROP diagnosis means building an image stitching pipeline.
the good news
we came in at $155 against a $500 budget. that leaves a lot of headroom for the next team to put real money into the lens or a better sensor without breaking the affordability goal.
recommendations for the next team
- prioritize clinical validation. get IRB approval and capture images on real dilated infant eyes, that's the single biggest unknown.
- run formal user studies. we got informal feedback from judges and an ophthalmologist; the next team should run structured surveys with target users before further design changes.
- refine off-axis lighting or look for cheap coaxial alternatives. tune the front ring angle, try the included edmund optics glass cable, or find a beamsplitter approach that doesn't cost thousands.
- hardware swap for the focus distance. look at sensors with shorter minimum focus distances to reclaim the wasted internal length.
- spend some of the budget headroom. $345 of room: a higher quality lens (~$500) might be worth it; partnering with thorlabs or edmund optics could bring that down.
handoff
we already delivered a demonstration to our client, katherine sammy, walked her through the device, and showed her the poster. all four of us would love to help the next team that picks this up.
team retinex
samer marmash, alisha sankhe, teo kakabadze, clin vadakkal shaiju EDES 200 engineering design, rice university.
client: katherine sammy · sponsor: harrell huff · mentors: dr. oden, dr. hunter, dr. ghosn, dr. emmanuel chang. support: oshman engineering design kitchen + donations from thorlabs and edmund optics.
← back to projects